What Canadian Families Should Know About Hospice Care and Advocacy
Article Written by Bob Shannon
For Canadian families facing hospice care for the first time, the hardest part is how fast everything gets serious while everyone is still trying to stay steady. The emotional challenges of hospice can hit all at once: grief, guilt, relief, and confusion, and those feelings don’t wait for anyone to feel “ready.” At the same time, practical hospice preparation shows up in real-world questions about comfort, choices, and who gets a say when decisions feel loaded. Add end-of-life care awareness and ongoing worries about euthanasia policies, oversight, and mental health supports, and it’s easy for supporting loved ones to feel overwhelmed.
Understanding Hospice Care and When to Call
Hospice care is a philosophy of care that puts comfort, dignity, and quality of life first when an illness is no longer responding to cure-focused treatment. The big shift is the goal: palliative care can happen alongside treatment, while hospice is usually for the last season of life, often when a doctor believes there may be six months or less to live if the illness follows its usual path.
This matters because knowing the difference helps families ask for the right supports early, not in a crisis. It also keeps advocacy grounded: when a good hospice is in place, people are less likely to feel pushed toward assisted death out of fear, pain, or burnout.
A simple rule of thumb is to call when comfort needs are rising fast, hospital trips are piling up, or daily care is becoming too much at home. Think of hospice like switching from “fixing the disease” to “protecting the person,” with a team built around relief and steady guidance.
With that clear, it helps to know the key terms and who to call for what.
Key Hospice Terms Canadian Families Should Know
These definitions make it easier for Canadian families to ask the right questions, reach the right person fast, and advocate for comfort-focused care without feeling steered toward assisted death. Knowing who does what also helps you document concerns clearly and keep decisions grounded in your loved one’s values.
● Hospice care: A team approach that focuses on comfort and support near the end of life, helping reduce crisis visits and pressure-filled decisions.
● Palliative care nurse: A nurse who manages symptoms like pain or nausea and teaches caregivers what to watch for at home.
● Hospice physician: A doctor who adjusts comfort medications, reviews goals of care, and supports clear, informed medical decisions.
● Social worker: A helper for emotional support, family meetings, benefits paperwork, and finding community resources during stress.
● Care coordinator: The person who schedules services, connects providers, and keeps the plan organized as needs change.
● Goals of care: A shared plan for what matters most, guiding choices about treatments, transfers, and comfort measures.
● Informed consent: Clear understanding of options, risks, and supports, so decisions reflect the patient’s wishes and not fear or isolation.
Next, we will compare home and facility-based hospice options in Canada. Now that these terms are clear, applying them will feel much easier.
Hospice Care Settings Compared at a Glance
This table compares common hospice and palliative settings Canadians may be offered, so you can choose the level of support that fits your family’s capacity and your loved one’s values. Clarity matters because when care feels unstable or under-supported, families can feel pushed into rushed decisions, instead of steady comfort care and informed consent.
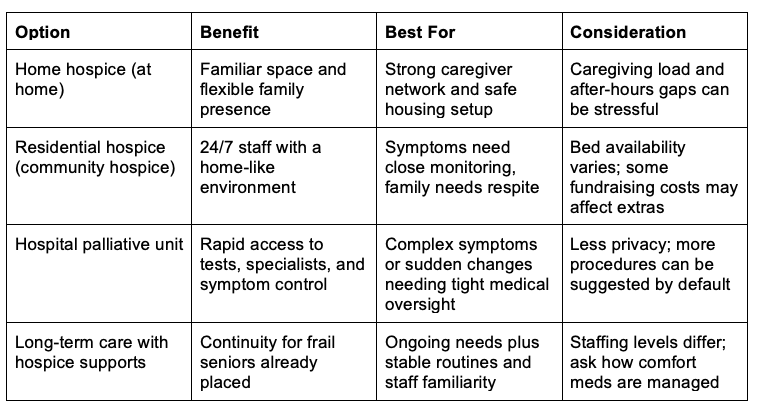
If you are choosing between settings, start by mapping what is non-negotiable: symptom control, calm communication, and time to decide without pressure. Then ask what support arrives overnight and on weekends, since that is where crises often start. Knowing which option fits best makes your next move clear.
Next, we will tackle the most common questions about comfort measures, costs, and patient rights.
Common Hospice Questions, Answered Simply
Q: What exactly is hospice care and why is it considered necessary for a loved one nearing end of life?
A: Hospice is comfort-focused care when treatment is no longer helping, with an emphasis on pain relief, dignity, and steady support. It can lower panic during crises because there is a plan and a team to call. It also protects patient rights by centering informed consent and resisting rushed, irreversible choices.
Q: When is the appropriate time to contact hospice services for my family member?
A: Reach out when symptoms are escalating, caregiving is getting shaky overnight, or your loved one keeps landing in urgent care. Calling early does not mean “give up,” it buys time, options, and calmer decision-making. Ask what is covered and what may be extra, since hospice care at home can involve high private costs for intensive support.
Q: Who are the members of the hospice care team, and what roles do they play in supporting my loved one?
A: Teams often include a nurse, doctor, social worker, spiritual care, and volunteers, plus pharmacy and personal support, depending on the setting. The nurse manages symptoms and teaches the family what to watch for; the social worker helps with benefits, consent, and conflict. You can ask for one point person to reduce mixed messages and stress.
Q: What practical ways can I help keep my loved one comfortable during their time in hospice?
A: Keep a simple symptom log for pain, breathlessness, nausea, and agitation, then share it at each visit. Ask about mouth care, gentle repositioning, quiet lighting, and medication timing to prevent spikes. If anything feels pressured, request a pause for explanation and written consent before changes.
Q: How can I organize and manage the complex paperwork and decisions involved in arranging hospice care to reduce my stress?
A: Start by listing what you already have: health card details, medication list, substitute decision-maker papers, advance directives, and recent discharge notes. Put everything into one labelled folder, merge and rename PDFs with online PDF tools, then share a single updated package with the hospice nurse, the main family contact, and any legal decision-maker. A clear plan of care helps you confirm what services were agreed to and what needs a new signature.
Small, steady steps protect comfort care and keep uncertainty from running the show.
Advocate for Comfort and Consent in Canadian Hospice Care
Hospice can feel like a blur of paperwork and pressure, especially when end-of-life choices and euthanasia debates are in the background. The steadier path is informed hospice decision-making: keep the focus on supportive end-of-life care, ask plain-language questions, and treat advocacy for hospice patients as a shared family role, not a confrontation. When that mindset leads, care plans stay clearer, ethical considerations in hospice care get named early, and your loved one’s wishes are less likely to be sidelined. Comfort and consent should guide every hospice decision. Ask your hospice team to confirm, in writing, the current goals of care and who is authorized to speak and sign. That kind of clarity builds trust and resilience for everyone walking this part of the road together.
Article author Bob Shannon may be reached at bob@seniorsmeet.org
More Stories and Articles









